Persons with diabetes are at risk of chronic limb-threatening ischaemia. While treating ischaemia is crucial, care beyond surgical treatment is also crucial to recovery. We share how a customised approach with a multidisciplinary team is the best approach to the disease.
INTRODUCTION
Diabetes mellitus has increased in prevalence over
the years and now affects 400 million globally.1
Diabetic patients are at risk of chronic limb-threatening ischaemia (CLTI) as 25% of them develop a foot ulcer, and 80% of major amputations begin as one.1
Many may not experience classic rest pain or prior
claudication, and have a falsely raised ankle-brachial
index. Poor perfusion, peripheral neuropathy
and immunocompromised states lead to delayed
presentation, extensive wounds and infections which
render limbs unsalvageable.
While people are increasingly familiar with the diabetic
foot from the media, relatives and friends, delayed
presentation is common due to the initial ignorance or
unnoticed tissue trauma. Others lack proper foot care,
education and surveillance.
CLTI is part of a broad disease spectrum where treating
ischaemia, while crucial, is only one determinant
of success. Through a case study, this article hopes
to show that customised treatment taken on by a
multidisciplinary team is the best approach to the
disease.2
BACKGROUNDMr A was 55 years old and a smoker of 30 pack-years,
with a body mass index (BMI) of 32. He had been diabetic for five years (HbA1c 10.2%)
and underwent coronary bypass at 54 years of age.
He has stage 3 kidney disease and an incidental
asymptomatic left carotid stenosis for which he
declined intervention. Presentation
He presented with wet gangrene of his right second
to fourth toes, associated with fever and hypotension
three weeks after he knocked his toes during a brief
syncopal episode. 
Amputation
Mr A underwent emergent second-to-fifth-toe ray
amputation with a plantar slit to allow drainage of
purulent infection. His fifth toe was involved and had
osteomyelitis on radiograph. 
Post-debridement
Imaging
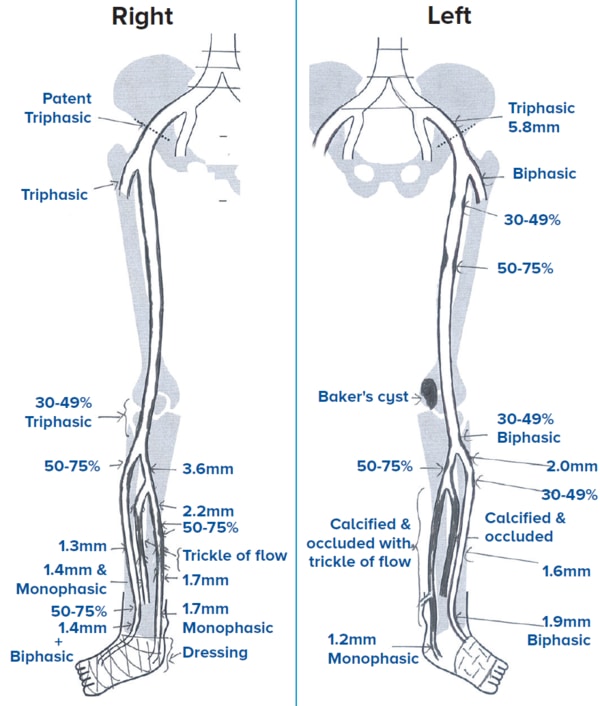
Being a smoker with poorly-controlled diabetes, Mr
A’s lower limb arterial duplex showed multi-level
calcified steno-occlusive disease of the common
femoral artery (CFA), superficial femoral artery (SFA)
and below-the-knee (BTK) tibial disease. He had a
toe pressure measurement of 15 mmHg. 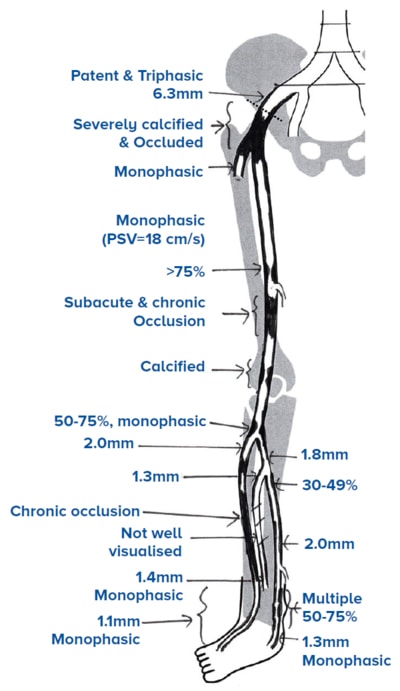
Ultrasound
arterial
duplex of
Mr A’s right
lower limb |
In stable patients, it is preferable to do same-setting
revascularisation and amputation. However,
when in septic shock, time is of the essence and
the removal of the septic source must not be delayed.

CLTI may also present as ulcers or abscesses in
web spaces and pressure areas from ill-fitted
footwear.
Long segment and small BTK tibial vessel disease
with poor-to-no below-ankle perfusion is typical of
CLTI patients.
TECHNICAL CONSIDERATIONS IN IMAGING
AND SURGERY
Angioplasty rather than bypass is the mainstay
of treatment, but without established target outflow,
primary amputation to an infection-free, well-perfused
level may be the only option.
Use of imaging to guide treatment
In patients without a palpable femoral pulse and when
the proximal inflow cannot be assessed on ultrasound,
a computed tomography scan or magnetic resonance
aortoiliac is required.
Concomitant aortic or proximal disease can be
visualised and determines whether a contralateral
retrograde or upper limb access is necessary for
angioplasty.
In severely stenotic or occluded CFA disease, an
open endarterectomy is preferred for a hybrid openendovascular procedure. It is thus useful to identify a
non-calcified proximal ‘clamp-able’ segment and its
relation to the inguinal ligament preoperatively for
open surgery.
Imaging can also show acute or subacute features
where thrombolysis or thrombectomy with aspiration
devices may be required.
Contrast use for imaging and angioplasty may worsen
renal function. This can be minimised with the use of
carbon dioxide for angiograms, pre-surgery hydration
and avoidance of nephrotoxic agents.
Endovascular therapy
Endovascular therapy is well-established for lower
limb revascularisation.3
A sheath is placed in an access vessel under ultrasound
guidance (usually CFA) and a digital subtraction
angiogram (DSA) is performed. Intra-arterial heparin is
administered and wires are used to transverse vessel
lesions so as to deploy balloon(s) across.
Balloon insufflation establishes lumen, treating the
stenosis or occlusion.
SAFARI technique
In long segment disease, it is sometimes necessary to
employ a subintimal arterial flossing with antegrade-retrograde
intervention (SAFARI) technique where
‘true lumen’ percutaneous access from two directions
is used to ‘cross a lesion’ to obtain a through and
through passage.
Increasingly, atherectomy devices are used to achieve
luminal gain before balloon angioplasty to reduce
vessel dissection.
Stenting
Stenting is necessary when there is significant or
persistent vessel recoil, dissection, high clot burden
and perforation. They are costly and surveillance is
required as they can re-stenose or occlude over time.
Data for and against drug elution technology
(paclitaxel- or sirolimus-based) exist.4 These are
generally used for short-interval recurrent disease
and may add duration to vessel patency.
Angioplasty
Angioplasty aims to provide straight-line flow to the
wound that is ideally angiosome based, or to re-establish
a plantar arch when possible.
Bypass
When flow cannot be achieved in an interveningmsegment (e.g., SFA) or in stent failure, a bypass option
with native vein or graft is possible.
Bypass procedures have higher perioperative risks,
longer operative times and hospital stays. They are at
risk of wound and graft infections and are subjected
to the availability of conduits such as native veins.Native-vein, above-tibial bypasses have the best long-term
results.
Bypasses are performed for fitter patients with
reasonable premorbid ambulatory status and cardiac
ejection fraction.
SURGERYMr A underwent a hybrid procedure consisting of an open common femoral endarterectomy, followed by
a bovine patch repair. A sheath was then placed antegrade into the patch to perform the angiogram and
angioplasty of the infrainguinal vessels. 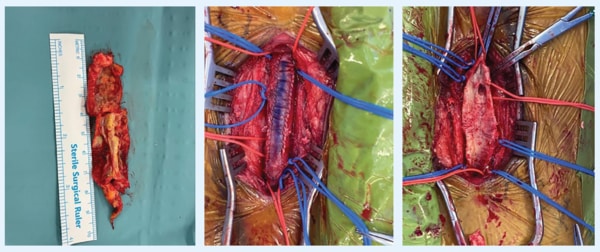
Femoral endarterectomy
and patch repair along with
removed calcified plaque 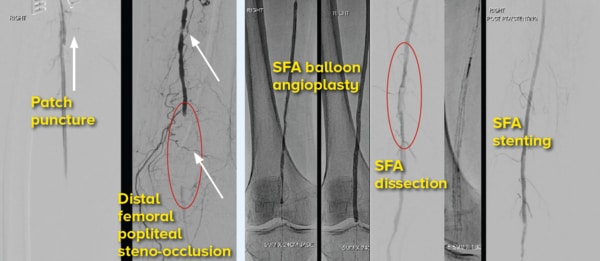
Angiographic images showing
CFA patch puncture, femoral
popliteal disease, balloon
dissection, stent deployment and restored flow 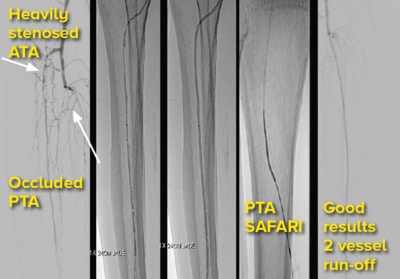
BTK-anterior tibial angioplasty (ATA), posterior
tibial artery (PTA) SAFARI 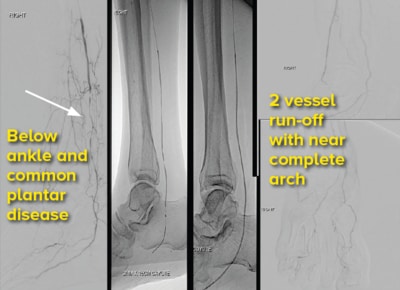
Distal percutaneous transluminal angioplasty and
common plantar angioplasty |
WOUND HEALING AND RECOVERY
Monitoring and care
Wound healing requires appropriate culture-directed antibiotics, avoidance of new trauma, maintaining perfusion and optimising care of existing cardiac, renal, glycaemic, ambulatory and nutritional status, while going through ongoing rehabilitation.
Prolonged stays with immobility lead to the development of pressure sores and nosocomial infections, and must be avoided.
The antibiotic duration depends on wound progress and the presence of existing infections such as osteomyelitis or bacteraemia. Inflammatory markers are useful adjuncts and an infectious diseases physician is often consulted.
Vascular access lines may be needed when prolonged treatment is required, but pose a threat when infected and require frequent examination.
Repeat angioplasty may be needed if wound healing is impaired.
Vascular teams, along with dedicated wound nurses and podiatrists, perform regular wound inspections, debridement and dressing changes.
A variety of dressing options including antiseptic solutions, cellulose/collagen-based dressings, hydrocolloids, vacuum-assisted closure devices and hyperbaric therapy or oxygen delivery devices are available for different types of wounds.
Continued wound care
Continued wound care is paramount for success, and step-down facilities such as community hospitals, day care and home nursing facilitate rehabilitation till patients or caregivers are confident to be independent at home.


Recovery of heel and pressure wounds
Heel and pressure wounds are challenging as blood flow is poor and offloading, despite best efforts, may not be possible due to immobility.
Wounds after revascularisation are in a race against time as they have a risk of reinfection or deterioration.
Those that granulate well and have been treated for infection should pursue coverage in the form of skin graft or flap performed by either vascular or plastic surgery.

Recovery from major limb amputation
A timely decision to perform amputation will save lives. However, acceptance can be stressful and requires dedicated physicians, social workers and rehabilitation teams.
When the stump heals, many enjoy sepsis-free, excellent quality of life with earlier return to society and eventual prosthesis fitting.

RECOVERYMr A’s wound healed well with split skin graft and he regained reasonable ambulation after six months. Two years on, he required a below-the-knee amputation of his other leg when he re-presented with heel gangrene and calcaneal osteomyelitis. Help was sought late due to depression and worries over job commitments. He eventually required hemodialysis as his kidneys failed. Fortunately, his forefoot remained well and he eventually learned to walk with a below knee prosthesis. He no longer has open wounds and is able to hold a clerical job. He gets around with a personal mobility device and most importantly, enjoys time with his grandchildren. |
THE DEPARTMENT OF VASCULAR SURGERY
AT SINGAPORE GENERAL HOSPITAL
The Singapore General Hospital Department of Vascular Surgery performs an average of 400 lower limb angioplasties a year and collaborates closely with the Department of Interventional Radiology.
A retrospective review of 3,303 angioplasty procedures performed on 2,402 limbs from 2005 to 2015 showed salvage rates of 75%, 72% and 62%, and overall survival rates of 79%, 56% and 34% at 1, 5 and 10 years respectively.5
The department performs open and hybrid procedures, manages wounds and treats a variety of renal, carotid and aortic conditions.
TAKE-HOME MESSAGES FOR GPs
A vascular consultation is always advised for CLTI.
The treatment varies depending on comorbidities,
activities of daily living function, extent of tissue loss,
as well as social background and personal beliefs and
attitudes. Limb salvage, while ideal, may not always be possible or permanent.
Many go through great physiological and psychological
ordeals, and expenses and caregiver stress put
a strain on relationships. Others may seek alternative
(harmful) therapy or slide into depression.
GPs have preventive roles and can participate in
education, wound and emotional care.
REFERENCES
-
J.L. Mills Sr., M.S. Conte, D.G. Armstrong, F.B. Pomposelli, A. Schanzer, A.N. Sidawy, et al., Society for Vascular Surgery Lower Extremity Guidelines
Committee, The Society for Vascular Surgery lower extremity threatened limb classification system: risk stratification based on wound, ischaemia,
and foot infection (WIfI); J Vasc Surg, 59 (2014), pp. 220-234.e1-234.e2
- Chung J, Modrall JG, Ahn C, Lavery LA, Valentine RJ. Multidisciplinary care improves amputation-free survival in patients with chronic critical limb
ischaemia. J Vasc Surg. 2015 Jan;61(1):162-9. doi: 10.1016/j.jvs.2014.05.101. Epub 2014 Jul 26. PMID: 25073577.
- DeRubertis BG, Faries PL, McKinsey JF, Chaer RA, Pierce M, Karwowski J, Weinberg A, Nowygrod R, Morrissey NJ, Bush HL, Kent KC. Shifting
paradigms in the treatment of lower extremity vascular disease: a report of 1000 percutaneous interventions. Ann Surg. 2007 Sep;246(3):415-22;
discussion 422-4. doi: 10.1097/SLA.0b013e31814699a2. PMID: 17717445; PMCID: PMC1959357.
- Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Paraskevopoulos I, Karnabatidis D. Risk of Death and Amputation with Use of Paclitaxel-Coated
Balloons in the Infrapopliteal Arteries for Treatment of Critical Limb Ischaemia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Vasc Interv Radiol. 2020 Feb;31(2):202-212. doi: 10.1016/j.jvir.2019.11.015. Epub 2020 Jan 15. PMID: 31954604.
- Ni WW, Leong S, Irani F, Patel A, Damodharan K, Venkataranasimha N, Chandramohan S, Kumar P, Chua J, Gogna A, Da Zhuang K, Chong TT,
Tang TY, Chng SP, Tay KH. “Angioplasty-First” Approach for Limb Salvage in Asian Patients with Critical Limb Ischaemia: Outcomes from 3,303
Angioplasties on 2,402 Limbs in a Single Tertiary Hospital. J Vasc Interv Radiol. 2020 Dec;31(12):1969-1977.e1. doi: 10.1016/j.jvir.2020.08.008. Epub
2020 Nov 1. PMID: 33139186.
Dr Nick Ng Zhi Peng is an Associate Consultant at the Department of Vascular Surgery
in Singapore General Hospital. He graduated from the Yong Loo Lin School of Medicine,
National University of Singapore in 2011 and completed his surgical training with the
SingHealth General Surgery Residency Programme in 2018. He obtained his Masters of Medicine (Surgery) in 2017 and FRCS (Edinburgh) in March 2019. He has an interest in both
open and endovascular surgery and hopes to help patients with chronic limb threatening
ischaemia have the best possible quality of life.
GPs can call the SingHealth Duke-NUS Vascular Centre for appointments at the
following hotlines:
Singapore General Hospital: 6326 6060
Changi General Hospital: 6788 3003
Sengkang General Hospital: 6930 6000
KK Women’s and Children’s Hospital: 6294 4050
National Heart Centre Singapore: 6704 2222

